MIYO connects districts to a network of licensed providers and supports hybrid models with teletherapy.
We have no expertise in mental health, where do we begin?
MIYO provides structured pathways, guided workflows, and evidence-based practices that help districts confidently support student mental health, even without an in-house specialist team.
How is mental health different from SEL?
SEL builds skills for all students to thrive socially and emotionally.
Mental health support focuses on identifying needs, assessing risk, and providing tiered intervention.
MIYO bridges both worlds by giving clarity, screening tools, and decision support.
Why do we need universal screening?
Screening uncovers students who may otherwise go unnoticed.
With MIYO, screening is automated, bilingual, consent-linked, and integrated into referral workflows, enabling early support instead of reactive crisis management.
Our intake and referral processes are manual. Can MIYO help?
Yes. MIYO automates the entire workflow from intake to risk scoring, assignment and follow-up ensuring cases move forward smoothly without email chains, paper tracking, or lost information.
Can we use our own consent forms?
Absolutely. District-approved consent templates can be uploaded and used digitally with secure e-signature tracking inside MIYO.
Can we use our own custom intake forms?
Yes. MIYO includes a flexible form builder that allows districts to create custom intake formats, add conditional logic, and route forms automatically to the right team members.
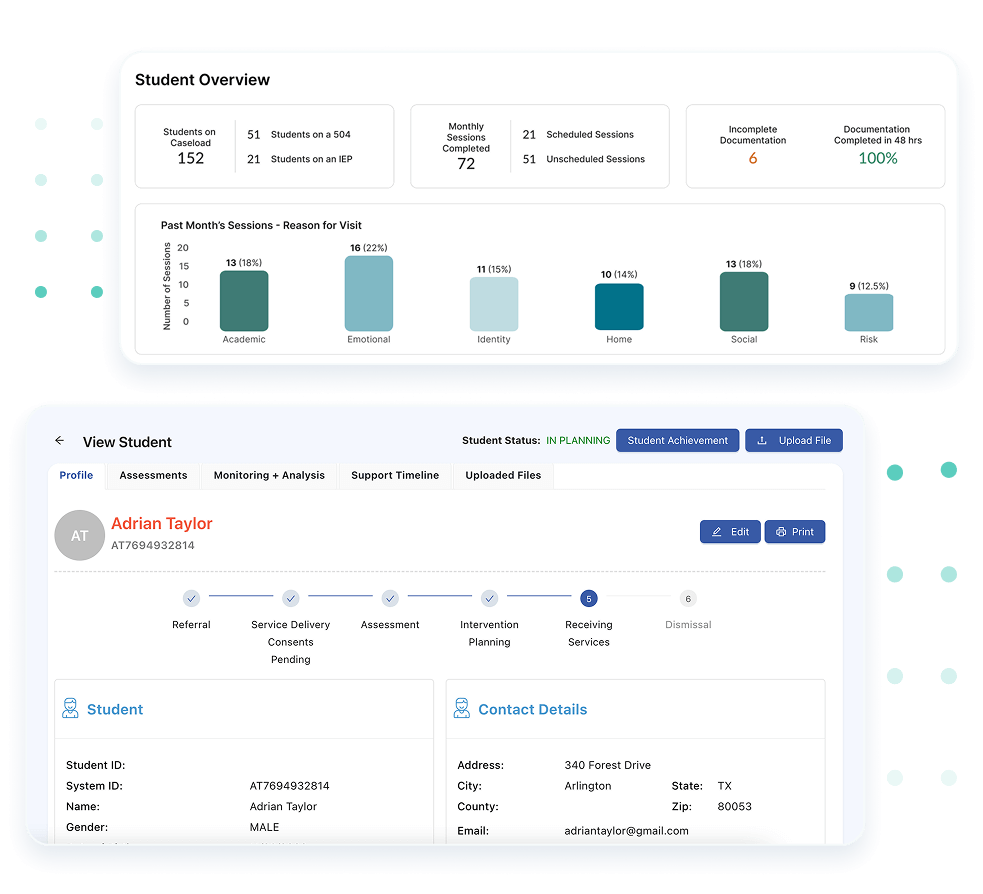
Our school counselors spend 2 hours manually pulling data from 5+ systems to
prepare for a parent meeting, can MIYO help?
MIYO centralizes everything student history, screenings, notes, consents, referrals, interventions, communication, into a single student file accessible in seconds.
We know we need more resources and a better platform, where do we find funding?
With MIYO, districts generate measurable data (needs, caseloads, outcomes) that strengthens funding proposals, supporting grant applications and state-aligned funding pathways.